Tuesday December 19, 2006
Something to share !
Today we will take a little break to share this important statement:
"As you learn to become a doctor, there is a frequent sense of surprise, a feeling that you are not entitled to the kind of intrusion you are allowed into patients' lives. Without arguing, they permit you to examine them; it is impossible to imagine, when you do your very first physical exam, that someday you will walk in calmly and tell a man your grandfather's age to undress, and then examine him without thinking about it twice. You get used to it all, but every so often you find yourself marveling at the access you are allowed, at the way you are learning from their bodies, the stories, the lives and deaths of perfect strangers. They give up their privacy in exchange for some hope - sometimes strong, sometimes faint - of the alleviation of pain, the curing of disease. And gradually, with medical training, that feeling of amazement, that feeling that you are not entitled, scars over. You begin to identify more thoroughly with the medical profession - of course you are entitled to see everything and know everything; you're a doctor, aren't you? And as you accept this as your right, you move further from your patients, even as you penetrate more meticulously and more confidently into their lives."
- Perri Klass, M.D.
Read more about Dr. Klass here - source nih.gov
Monday, August 21, 2006
Monday August 21, 2006
THAM
Introduction; In patients with acute respiratory distress syndrome (ARDS), permissive hypercapnia is a strategy to decrease airway pressures to prevent ventilator-induced lung damage by lowering tidal volumes and tolerating higher arterial carbon dioxide tension. A pure respiratory acidosis generally does not require alkali therapy. Alkali therapy is indicated for either a metabolic acidosis or a mixed acidosis. The choice of buffer is based on type of acidosis, cardiorespiratory status, and lung mechanics.
Problem with NaHCO3: Slow infusions of NaHCO3 can be used to treat non-anion gap metabolic acidosis and some forms of increased anion gap acidosis. But using NaHCO3 to treat type A (hypoxia-related) lactic acidosis can be hazardous, particularly under conditions of hypoxemia, inadequate circulation, and limited alveolar ventilation.
THAM: Under above circumstances, THAM is the preferable buffer because it does not increase PaCO2 and is excreted by the kidneys. Tromethamine (THAM) is a sodium-free alkalinizing agent that acts as a hydrogen ion (proton) acceptor. It is a weak base that combines with hydrogen ions from carbonic acid to form bicarbonate and cationic buffer. Administration of tromethamine decreases hydrogen ion concentration, which results in a decrease in carbon dioxide concentrations and an increase in bicarbonate concentrations. The administration of Tham also increases urine output through osmotic diuresis. Excretion of electrolytes and CO2 is also increased. Urine pH is raised along with the excretion of electrolytes.
Usual Dose:
Dose in ml's of 0.3M THAM = (1.1) (Wt. in Kg) (normal HCO3 – Pt’s HCO3)
OR
Dose in ml’s of 0.3M THAM = body wt in kg X base deficit in MEq/L x 1.1
Total dose should be administered over a period not less than 1 hour via central line.
.3M THAM solution is available as premix and is contra-indicated in renal failure, anuria and hyperkalemia. It may cause transient hypoglycemia and respiratory depression.
THAM
Introduction; In patients with acute respiratory distress syndrome (ARDS), permissive hypercapnia is a strategy to decrease airway pressures to prevent ventilator-induced lung damage by lowering tidal volumes and tolerating higher arterial carbon dioxide tension. A pure respiratory acidosis generally does not require alkali therapy. Alkali therapy is indicated for either a metabolic acidosis or a mixed acidosis. The choice of buffer is based on type of acidosis, cardiorespiratory status, and lung mechanics.
Problem with NaHCO3: Slow infusions of NaHCO3 can be used to treat non-anion gap metabolic acidosis and some forms of increased anion gap acidosis. But using NaHCO3 to treat type A (hypoxia-related) lactic acidosis can be hazardous, particularly under conditions of hypoxemia, inadequate circulation, and limited alveolar ventilation.
THAM: Under above circumstances, THAM is the preferable buffer because it does not increase PaCO2 and is excreted by the kidneys. Tromethamine (THAM) is a sodium-free alkalinizing agent that acts as a hydrogen ion (proton) acceptor. It is a weak base that combines with hydrogen ions from carbonic acid to form bicarbonate and cationic buffer. Administration of tromethamine decreases hydrogen ion concentration, which results in a decrease in carbon dioxide concentrations and an increase in bicarbonate concentrations. The administration of Tham also increases urine output through osmotic diuresis. Excretion of electrolytes and CO2 is also increased. Urine pH is raised along with the excretion of electrolytes.
Usual Dose:
Dose in ml's of 0.3M THAM = (1.1) (Wt. in Kg) (normal HCO3 – Pt’s HCO3)
OR
Dose in ml’s of 0.3M THAM = body wt in kg X base deficit in MEq/L x 1.1
Total dose should be administered over a period not less than 1 hour via central line.
.3M THAM solution is available as premix and is contra-indicated in renal failure, anuria and hyperkalemia. It may cause transient hypoglycemia and respiratory depression.
Thursday, August 10, 2006
Thursday August 10, 2006
Level of central line tip may predispose to thrombosis
Interesting retrospective review of 428 central lines (inserted into 334 patients) was done in UK to look into the level central line tip's relation to thrombosis 1. The median follow-up was 72 days.
* The chest radiograph obtained post-catheter insertion, as well as follow-up radiographs, linograms, venograms and Doppler ultrasounds (US), were reviewed.
They found that: "There was a significant difference in thrombosis rate between lines sited with the tip in a distal third of the superior vena cava (2.6%) compared with a proximal third of the superior vena cava (41.7%) - CVC with tips in a proximal position were 16 times more likely to thrombose than those in a distal position".
Related previous pearls:
CXR reading for optimum tip of central line
and
What if SC central line ends up in IJ vein?
Reference:
1. To clot or not to clot? That is the question in central venous catheters - Clinical Radiology, Volume 59, Issue 4, April 2004, Pages 349-355
Level of central line tip may predispose to thrombosis
Interesting retrospective review of 428 central lines (inserted into 334 patients) was done in UK to look into the level central line tip's relation to thrombosis 1. The median follow-up was 72 days.
* The chest radiograph obtained post-catheter insertion, as well as follow-up radiographs, linograms, venograms and Doppler ultrasounds (US), were reviewed.
They found that: "There was a significant difference in thrombosis rate between lines sited with the tip in a distal third of the superior vena cava (2.6%) compared with a proximal third of the superior vena cava (41.7%) - CVC with tips in a proximal position were 16 times more likely to thrombose than those in a distal position".
Related previous pearls:
CXR reading for optimum tip of central line
and
What if SC central line ends up in IJ vein?
Reference:
1. To clot or not to clot? That is the question in central venous catheters - Clinical Radiology, Volume 59, Issue 4, April 2004, Pages 349-355
Wednesday, August 09, 2006
tip of central line
Saturday July 22, 2006
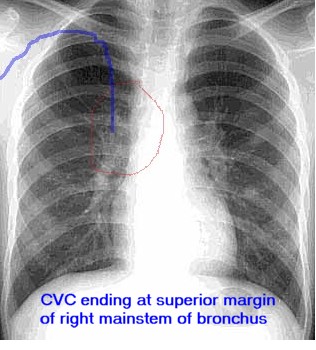
Do you need to pull back the central line?
Ideally, tip of central venous catheter should not lie in cardiac structures and the desirable position is mid superior vena cava.
Simple tip: If the tip of central venous catheter is above the superior margin of Right mainstem bronchus, it is unlikely to be in atrium.
Friday, July 21, 2006
Friday July 21, 2006
Prohibiting cell phones in ICUs - Are we over-reacting !
Truely speaking, there have been no studies to determine the harm or benefit of mobile/cell phones in ICUs. Generally, cell phones are prohibited in hospitals, particularly in ICUs and telemetry floors due to concern of EMI* with pacemakers, ventilators, infusion pumps and other electronic units. It became pretty standard with a report published about 12 years ago 1.
* EMI = electromagnetic interference
At the 2003 meeting of the ASA (American Society of Anesthesiologists), 7878 five-questions survey, regarding modes of communication in the ORs/ICUs, were distributed. 4018 responses were received 2.
Prohibiting cell phones in ICUs - Are we over-reacting !
Truely speaking, there have been no studies to determine the harm or benefit of mobile/cell phones in ICUs. Generally, cell phones are prohibited in hospitals, particularly in ICUs and telemetry floors due to concern of EMI* with pacemakers, ventilators, infusion pumps and other electronic units. It became pretty standard with a report published about 12 years ago 1.
* EMI = electromagnetic interference
At the 2003 meeting of the ASA (American Society of Anesthesiologists), 7878 five-questions survey, regarding modes of communication in the ORs/ICUs, were distributed. 4018 responses were received 2.
- 65% of surveyed reported using pagers as their primary mode of communications,
- 17.5% of surveyed reported using cell-phones as their primary mode of communications and
- 17.5% used overhead paging (or did not respond to this question)
And
- Among the 2607 respondents using pagers, 1179 (45%) reported experiencing significant delays in communication and 407 indicated that these delays led to medical error or patient injury.
- 31% of cell-phone users reported delays in communications.
- Only 2.4% of the respondents indicated that they had ever experienced interference between a cell phone and a medical device.
It has been suggested that through proper policy controls, hospitals can provide a more safe environment taking advantage of this 2-way communication technology, with a reduction in the risk of medical error or injury resulting from delay !!.
It has been recommended that as far as cell phones be kept at least 1 meter away from medical equipment, they seems safe 3.
Similar theme was echoed in an editorial in BMJ about 3 years ago: Mobile phones in hospitals (BMJ 2003;326:460-461 - 1 March)
Related previous pearl: Noise level in ICUs
References: click to get abstract/article
1. Mobile telephones interfere with medical electrical equipment - Australas Phys Eng Sci Med.1994 Mar;17(1):23-7.
2. Communication in Critical Care Environments: Mobile Telephones Improve Patient Care - Anesth Analg 2006;102:535-541
3. Modern Wireless Telecommunication Technologies and Their Electromagnetic Compatibility with Life-Supporting Equipment - Anesth Analg 2005;101:1393-1400
Thursday July 20, 2006
Q: what is "cryo reduced plasma"?
A; Yesterday we learned that: one unit of cryoprecipitate is derived from one unit of fresh frozen plasma (FFP). Left over FFP, after removal of cryoprecipitate is called supernatant plasma or CRYO-REDUCED PLASMA.
Clinical Significance: Cryo-reduced plasma is used as a treatment in plasmapheresis for TTP, not responding to regular plasma exchange with FFP. Some physicians even use it as first line for plasmapheresis/Therapeutic Plasma Exchange (TPE) for a patient with Thrombotic Thrombocytopenic Purpura (TTP).
Wednesday, July 19, 2006
Wednesday July 19, 2006
Q: Why we call it cryoprecipitate?
A: The name explains everthing. cryoprecipitate means "cold precipitate". When FFP is thawed slowly at 4 degree C, a white precipitate forms at the bottom of the bag, which can then be separated from the supernatant plasma. This precipitate is rich in fibrinogen, factor VIII, von Willebrand factor, factor XIII, and fibronectin - and call crayoprecipitate. One unit of cryoprecipitate is derived from fresh frozen plasma (FFP) prepared from a unit of whole blood and as it is only a little precipitate at the bottom of the bag, 1 unit of cryoprecipitate comprised only a volume of 10-20 mL.
Contents:
Q: Why we call it cryoprecipitate?
A: The name explains everthing. cryoprecipitate means "cold precipitate". When FFP is thawed slowly at 4 degree C, a white precipitate forms at the bottom of the bag, which can then be separated from the supernatant plasma. This precipitate is rich in fibrinogen, factor VIII, von Willebrand factor, factor XIII, and fibronectin - and call crayoprecipitate. One unit of cryoprecipitate is derived from fresh frozen plasma (FFP) prepared from a unit of whole blood and as it is only a little precipitate at the bottom of the bag, 1 unit of cryoprecipitate comprised only a volume of 10-20 mL.
Contents:
- 80-100 units of factor VIII, which consists of both the procoagulant activity and the von Willebrand factor,
- 150-250 mg of fibrinogen,
- 50-100 units of factor XIII, and
- 50-60 mg of fibronectin.
Half life is about one year if stored at -18 degree C. When ordered (generally given as 6 units at a time), cryoprecipitate is thawed back to 37 degree C. Once thawed it must be kept at room temperature and has an expiration time of 4 to 6 hours.
Previous related pearls: How much FFP? and Some facts about FFP
Monday, July 17, 2006
Tuesday July 18, 2006
Q: How IV (intravenous) DDAVP (desmopressin) should be given?
A: DDAVP, short name of 1-deamino-8-D-arginine vasopressin and also known as desmopressin is use for varity of reasons in ICUs including uremic bleeding diasthesis, some platelet disorders, to boost the plasma level of factor VIII and von Willebrand factor (VWF) and in diabetes insipidus. It may be given as nasal spray or subcutaneous injection but in ICUs mostly get administrated via IV route.
DDAVP should be diluted in 100 ml of normal saline and given by slow intravenous infusion over 30 minutes. The usual dose is 0.3 mcg/kg. Rapid infusion may result in tachycardia, flushing, tremor and abdominal discomfort. Also thrombosis and even myocardial infarction after an infusion of DDAVP has been reported and should be used with caution in patients with signs of arterial disease.
Q: How IV (intravenous) DDAVP (desmopressin) should be given?
A: DDAVP, short name of 1-deamino-8-D-arginine vasopressin and also known as desmopressin is use for varity of reasons in ICUs including uremic bleeding diasthesis, some platelet disorders, to boost the plasma level of factor VIII and von Willebrand factor (VWF) and in diabetes insipidus. It may be given as nasal spray or subcutaneous injection but in ICUs mostly get administrated via IV route.
DDAVP should be diluted in 100 ml of normal saline and given by slow intravenous infusion over 30 minutes. The usual dose is 0.3 mcg/kg. Rapid infusion may result in tachycardia, flushing, tremor and abdominal discomfort. Also thrombosis and even myocardial infarction after an infusion of DDAVP has been reported and should be used with caution in patients with signs of arterial disease.
Monday July 17, 2006
Intensivists' compensation
We looked into recent surveys' from different sources and found the following:
* All compensations in US dollar annually
* K = 1000
Average base salary compensation for intensivist has been ranged from annual 195K (new graduate) to 240K (3/5 years experienced). Highly experienced intensivist (15-20 years) should have compensation around 255K - 263K annual.
Latest market: all these surveys were published atleast a year ago and in last 12 months advertisements for intensivists' opportunities continue to show rising trend of salaries even upto 225-250K for new graduates.
Academic factor: Intensivist at a university setting make less but have better life style due to house staff availability and protected time for research (average 168 K), while critical care staff physicians employed by a non-university-affiliated hospital gets higher compensation (avaerage 240K) but more burn out.
Total clinical time in university setting is around 26-34 weeks per year but in private groups it all depends on local needs with 40-47 weeks (with 4 weeks vacation and one week for CME). Many groups prefer to work in block scheduling (like '7 days on 7 days off' to wear off burn out).
VA factor: VA system intensivits have good benefits and life style (like their university based colleagues) but salary remained low around 130-140K 3. Recently, there are strong indications that salaries would go up.
eICU factor: Recently eICU physicians have been offered higher than average compensation with heavy investments in this sector from major health systems but still very few intensivists have been found to take it as a full time employment.
Subspeciality factor: Overall critical care anesthesiologists and critical care non-trauma surgeons were under-compensated per one survey 1. Out of all PEDIATRIC intensivists found to be in highest demand due to lowest supply.
Geographical: Region wise east coast (particularly north east) has about 5-10% less compensation in all fields as compared to other regions.
Benefits: Benefits and bonuses upto 15% on top of base salary is a norm. In benfits - continuing medical education (CME) allowance range from 1000 - 5000 per year with average of 3000 US annual. 401 K (retirement), ADD, life insurance are usually part of the package but 3 essential benefits should include
Mal-practice coverage: As a standard, malpractice with tail should be covered. New graduates often fail to ask for tail coverage and later found themselves in hot water with a condition call 'locked by the tail'. If candidate fail to negotiate but in later years want to relocate or leave the group, tail buying costs around 30K to 80K, depending on region. Tail buying is 200% of annual malpractice premiums.
Non-compete clause: Ideally, there should not be any non-compete or restrictive covenant clause as intensivists are unlikely to carry their own patient base but when private group is contracted or busy in one ICU its natural to have restrictive covenant and should be accepted as standard business practice.
References:
1. Compensation for Physicians in Critical Care - Compensation of Critical Care Professionals 2005 - Society of Critical Care Medicine
2. The 2005 AMGA (American Medical Group Association) Medical Group Compensation and Financial Survey - cejkasearch.com
3. Testimony of Dr. Stephen P. Rosenthal President National Association of VA Physicians and Dentists
4. Intensive care unit physician staffing: Financial modeling of the Leapfrog standard - Critical Care Medicine. Interface of Public Policy and Critical Care Medicine. 34(3) Suppl:S18-S24, March 2006.
Intensivists' compensation
We looked into recent surveys' from different sources and found the following:
* All compensations in US dollar annually
* K = 1000
Average base salary compensation for intensivist has been ranged from annual 195K (new graduate) to 240K (3/5 years experienced). Highly experienced intensivist (15-20 years) should have compensation around 255K - 263K annual.
Latest market: all these surveys were published atleast a year ago and in last 12 months advertisements for intensivists' opportunities continue to show rising trend of salaries even upto 225-250K for new graduates.
Academic factor: Intensivist at a university setting make less but have better life style due to house staff availability and protected time for research (average 168 K), while critical care staff physicians employed by a non-university-affiliated hospital gets higher compensation (avaerage 240K) but more burn out.
Total clinical time in university setting is around 26-34 weeks per year but in private groups it all depends on local needs with 40-47 weeks (with 4 weeks vacation and one week for CME). Many groups prefer to work in block scheduling (like '7 days on 7 days off' to wear off burn out).
VA factor: VA system intensivits have good benefits and life style (like their university based colleagues) but salary remained low around 130-140K 3. Recently, there are strong indications that salaries would go up.
eICU factor: Recently eICU physicians have been offered higher than average compensation with heavy investments in this sector from major health systems but still very few intensivists have been found to take it as a full time employment.
Subspeciality factor: Overall critical care anesthesiologists and critical care non-trauma surgeons were under-compensated per one survey 1. Out of all PEDIATRIC intensivists found to be in highest demand due to lowest supply.
Geographical: Region wise east coast (particularly north east) has about 5-10% less compensation in all fields as compared to other regions.
Benefits: Benefits and bonuses upto 15% on top of base salary is a norm. In benfits - continuing medical education (CME) allowance range from 1000 - 5000 per year with average of 3000 US annual. 401 K (retirement), ADD, life insurance are usually part of the package but 3 essential benefits should include
- Malpractice with tail coverage
- Health/dental benefits for self and family
- CME
Mal-practice coverage: As a standard, malpractice with tail should be covered. New graduates often fail to ask for tail coverage and later found themselves in hot water with a condition call 'locked by the tail'. If candidate fail to negotiate but in later years want to relocate or leave the group, tail buying costs around 30K to 80K, depending on region. Tail buying is 200% of annual malpractice premiums.
Non-compete clause: Ideally, there should not be any non-compete or restrictive covenant clause as intensivists are unlikely to carry their own patient base but when private group is contracted or busy in one ICU its natural to have restrictive covenant and should be accepted as standard business practice.
References:
1. Compensation for Physicians in Critical Care - Compensation of Critical Care Professionals 2005 - Society of Critical Care Medicine
2. The 2005 AMGA (American Medical Group Association) Medical Group Compensation and Financial Survey - cejkasearch.com
3. Testimony of Dr. Stephen P. Rosenthal President National Association of VA Physicians and Dentists
4. Intensive care unit physician staffing: Financial modeling of the Leapfrog standard - Critical Care Medicine. Interface of Public Policy and Critical Care Medicine. 34(3) Suppl:S18-S24, March 2006.
Sunday, July 16, 2006
Sunday July 16, 2006
Optimum patients' load for intensivist
ICUs in united stated range anywhere from 6 to 24 beds or may be more. At this point, it is not clear at what point intensivist's efficiency plateau out and effects the overall outcome.
Drs. Saqib Dara, MD and Bekele Afessa, MD from Division of Pulmonary and Critical Care Medicine, Mayo Clinic College of Medicine, Rochester, MN looked into the issue with regression analyses of about 25,00 patients. They divided intensivits' patients load into 4 groups:
Reference: click to get article/abstract
Intensivist-to-Bed Ratio - Association With Outcomes in the Medical ICU - chest. 2005;128:567-572.
Optimum patients' load for intensivist
ICUs in united stated range anywhere from 6 to 24 beds or may be more. At this point, it is not clear at what point intensivist's efficiency plateau out and effects the overall outcome.
Drs. Saqib Dara, MD and Bekele Afessa, MD from Division of Pulmonary and Critical Care Medicine, Mayo Clinic College of Medicine, Rochester, MN looked into the issue with regression analyses of about 25,00 patients. They divided intensivits' patients load into 4 groups:
- 1:7.5,
- 1:9.5,
- 1:12, and
- 1:15
They found that the ICU period with one intensivist for 15 beds had a longer adjusted ICU LOS (length of stay). Although the ICU period with an intensivist-to-bed ratio of 1:7.5 had the shortest ICU LOS ratio, the difference was not statistically significant compared to the periods with intensivist-to-ICU bed ratios of 1:9.5 or 1:12.
This is the only study of its kind from single institution but it appears that optimum number of patients, intensivist should carry to produce maximum outcome is around 12 or less.
It is all good work of intensivists' that observed ICU mortality did not differ significantly in any group despite progressive increase of load of work.
Reference: click to get article/abstract
Intensivist-to-Bed Ratio - Association With Outcomes in the Medical ICU - chest. 2005;128:567-572.
Saturday, July 15, 2006
Saturday July 15, 2006
Case: 32 year old male with history of HIV presented to ED with complaint of upper quadrant pain. Initial lab shows elevated LFT and severe acidosis with bicarb of 8 in initial chemistry. You quickly start working through your mnemonic of increased anion gap acidosis - "CAT MUD PILES" !! *. Lactic acid level reported 9.4 mg/dl. CT scan of abdomen done to rule out ischemic colitis but showed only hepatic steatosis. Patient clinically does not appears toxic or septic though you started him on IV fluid and prophylactic antibiotics. Pt. is ruled out for DKA and other causes of acidosis also. What is the probable source of his severe lactic acidosis ?
Answer: Cause is patient's HIV medicines (HAART - Highly Active Anti-Retroviral Therapy), mostly likely the nucleoside reverse-transcriptase inhibitors (NRTIs), - stavudine. NRTIs can cause hyperlactatemia by disrupting the function of the mitochondria. This is known as mitochondrial toxicity. NRTIs also cause fatty liver (hepatic steatosis), may be acute liver failure, and inefficient liver cannot metabolize lactic acid quickly resulting in severe hyperlactatemia.
This week The New England Journal of Medicine has posted a free article Intensive Care of Patients with HIV Infection (N Engl J Med 2006; 355:173-181, Jul 13, 2006).
* The mnemonic "CAT MUD PILES" is a easy way to remember the differential for an increased anion gap acidosis
Carbon monoxide, Cyanide,
Alcoholic ketoacidosis,
Toluene,
Methanol,
Uremia,
Diabetic ketoacidosis,
Paraldehyde, Phenformin,
Iron, Isoniazid,
Lactic acidosis,
Ethylene glycol,
Salicylates.
Case: 32 year old male with history of HIV presented to ED with complaint of upper quadrant pain. Initial lab shows elevated LFT and severe acidosis with bicarb of 8 in initial chemistry. You quickly start working through your mnemonic of increased anion gap acidosis - "CAT MUD PILES" !! *. Lactic acid level reported 9.4 mg/dl. CT scan of abdomen done to rule out ischemic colitis but showed only hepatic steatosis. Patient clinically does not appears toxic or septic though you started him on IV fluid and prophylactic antibiotics. Pt. is ruled out for DKA and other causes of acidosis also. What is the probable source of his severe lactic acidosis ?
Answer: Cause is patient's HIV medicines (HAART - Highly Active Anti-Retroviral Therapy), mostly likely the nucleoside reverse-transcriptase inhibitors (NRTIs), - stavudine. NRTIs can cause hyperlactatemia by disrupting the function of the mitochondria. This is known as mitochondrial toxicity. NRTIs also cause fatty liver (hepatic steatosis), may be acute liver failure, and inefficient liver cannot metabolize lactic acid quickly resulting in severe hyperlactatemia.
This week The New England Journal of Medicine has posted a free article Intensive Care of Patients with HIV Infection (N Engl J Med 2006; 355:173-181, Jul 13, 2006).
* The mnemonic "CAT MUD PILES" is a easy way to remember the differential for an increased anion gap acidosis
Carbon monoxide, Cyanide,
Alcoholic ketoacidosis,
Toluene,
Methanol,
Uremia,
Diabetic ketoacidosis,
Paraldehyde, Phenformin,
Iron, Isoniazid,
Lactic acidosis,
Ethylene glycol,
Salicylates.
Friday, July 14, 2006
SC CVC in IJ
Friday July 14, 2006
If SC central line ends up in IJ vein ?
It is always a possibility that central venous catheter placed in subclavian (SC) vein may take path upward and travel in internal jugular (IJ) vein. Incidence is about 5.4% and does not vary with side of insertion or with the head position during the procedure 1.
First 2 preventive measures,
1) One study clearly showed that if you direct 'tip of J-wire' caudally, the relative risk for cannulating the ipsilateral internal jugular vein is low 2.
OR
2) After cannulating subclavian vein, apply little pressure at ipsilateral IJ vein while passing wire. If wire stop threading or resistance felt, it means you need to pull back wire for few centimeters (making sure you don't loose vein cannulation) and thread again.
Alternatively, after you place subclavian catheter, before applying sutures there are 2 ways to make sure you are not in IJ vein.
1) Hook central line to central venous pressure (CVP) measurement. Apply firm pressure over the ipsilateral IJ vein in the supraclavicular region for approximately 10 seconds. Quick change in transducer pressure and waveform, like CVP increased by 5 mm Hg (fictitious rise in CVP) or flattening of waveforms indicates jugular misplacement of the catheter tip. Its called Internal Jugular Vein Occlusion Test 3.
OR
2) Flush about 3 -5 cc of saline and put your sthethoscope or even finger on ipsilateral IJ vein to hear or feel the bruit/flow.
In case, you don't do above maneuvers while inserting SC central line and CXR shows IJ placement, pull central venous cather back upto 4-5 cm from punture point and try above maneuvers. Another trick you can apply in case you have to pull back catheter and pass over J-wire again - thread J-wire only partially till you are sure you are in vein, pull back catheter completely (preferably use new catheter to avoid risk of infection) , slightly curve the tip of catheter downwards (like S tip PA-catheters) and pass with little twist.
References: Click to get abstract/article
1. Misplacement of subclavian venous Catheters: Importance of head position and choice of puncture site. BJA1990; 64: 632-33
2. Direction of the J-tip of the guidewire, in Seldinger technique, is a significant factor in misplacement of Subclavian vein catheter: A randomized, controlled study - Anesth Analg 2005;100:21-24
3. Internal Jugular Vein Occlusion Test For Rapid Detection Of Misplaced Subclavian Vein Catheter - The Internet Journal of Anesthesiology. 2005. Volume 9 Number 1
If SC central line ends up in IJ vein ?
It is always a possibility that central venous catheter placed in subclavian (SC) vein may take path upward and travel in internal jugular (IJ) vein. Incidence is about 5.4% and does not vary with side of insertion or with the head position during the procedure 1.
First 2 preventive measures,
1) One study clearly showed that if you direct 'tip of J-wire' caudally, the relative risk for cannulating the ipsilateral internal jugular vein is low 2.
OR
2) After cannulating subclavian vein, apply little pressure at ipsilateral IJ vein while passing wire. If wire stop threading or resistance felt, it means you need to pull back wire for few centimeters (making sure you don't loose vein cannulation) and thread again.
Alternatively, after you place subclavian catheter, before applying sutures there are 2 ways to make sure you are not in IJ vein.
1) Hook central line to central venous pressure (CVP) measurement. Apply firm pressure over the ipsilateral IJ vein in the supraclavicular region for approximately 10 seconds. Quick change in transducer pressure and waveform, like CVP increased by 5 mm Hg (fictitious rise in CVP) or flattening of waveforms indicates jugular misplacement of the catheter tip. Its called Internal Jugular Vein Occlusion Test 3.
OR
2) Flush about 3 -5 cc of saline and put your sthethoscope or even finger on ipsilateral IJ vein to hear or feel the bruit/flow.
In case, you don't do above maneuvers while inserting SC central line and CXR shows IJ placement, pull central venous cather back upto 4-5 cm from punture point and try above maneuvers. Another trick you can apply in case you have to pull back catheter and pass over J-wire again - thread J-wire only partially till you are sure you are in vein, pull back catheter completely (preferably use new catheter to avoid risk of infection) , slightly curve the tip of catheter downwards (like S tip PA-catheters) and pass with little twist.
References: Click to get abstract/article
1. Misplacement of subclavian venous Catheters: Importance of head position and choice of puncture site. BJA1990; 64: 632-33
2. Direction of the J-tip of the guidewire, in Seldinger technique, is a significant factor in misplacement of Subclavian vein catheter: A randomized, controlled study - Anesth Analg 2005;100:21-24
3. Internal Jugular Vein Occlusion Test For Rapid Detection Of Misplaced Subclavian Vein Catheter - The Internet Journal of Anesthesiology. 2005. Volume 9 Number 1
Wednesday, July 12, 2006
Wednesday July 12, 2006
Case: 47 year old morbidly obese female with baseline history of COPD, successfully extubated post-op and admitted to ICU for overnight observation after gastric bypass surgery. Patient appears more lethargic in late evening and ABG was drawn which showed PH of 7.20, PO2 of 59 and PCO2 of 98 (pt's baseline PCO2 is around 55). You ordered nebulizer treatments and applied full face mask's noninvasive positive pressure ventilation (BiPAP) with setting of 10/5 (IPAP of 10 cm H2O and EPAP of 5 cm H20) and ordered ABG after one hour. Followup ABG is PH of 7.24, PO2 of 72 and PCO2 of 86. Patient is still lethargic.Your next step would be:
A) Increase IPAP with followup ABG in 1-2 hours
B) Change to nasal mask with followup ABG in 1-2 hours
C) Intubate patient
D) Continue present settings with followup ABGin 1-2 hours
Answer: C
Noninvasive positive pressure ventilation (BiPAP) should be use with caution in fresh gastric bypass patients and there should be a low threshold to intubate if situation arise. BiPAP pumps air into the small gastric pouch and can lead to complications like breakdown of suture lines, bowel perforation and gastric distension. Though one small study of 27 patients didn't show either any complication or advantage of BiPAP in the first 24 postoperative hours of severely obese patients with comorbid illnesses who have undergone elective gastric bypass 1 but there are case reports in literature showing potential complication and geniune concern for use of of bi-level positive airway pressure after gastric bypass surgery 2.
Reference: click to get abstract/article
1.The effect of bi-level positive airway pressure on postoperative pulmonary function following gastric surgery for obesity - Respiratory Medicine Volume 96, Issue 9, September 2002, Pages 672-676
2. A potential complication of bi-level positive airway pressure after gastric bypass surgery - Obes Surg. 2004 Feb;14(2):282-4.
Case: 47 year old morbidly obese female with baseline history of COPD, successfully extubated post-op and admitted to ICU for overnight observation after gastric bypass surgery. Patient appears more lethargic in late evening and ABG was drawn which showed PH of 7.20, PO2 of 59 and PCO2 of 98 (pt's baseline PCO2 is around 55). You ordered nebulizer treatments and applied full face mask's noninvasive positive pressure ventilation (BiPAP) with setting of 10/5 (IPAP of 10 cm H2O and EPAP of 5 cm H20) and ordered ABG after one hour. Followup ABG is PH of 7.24, PO2 of 72 and PCO2 of 86. Patient is still lethargic.Your next step would be:
A) Increase IPAP with followup ABG in 1-2 hours
B) Change to nasal mask with followup ABG in 1-2 hours
C) Intubate patient
D) Continue present settings with followup ABGin 1-2 hours
Answer: C
Noninvasive positive pressure ventilation (BiPAP) should be use with caution in fresh gastric bypass patients and there should be a low threshold to intubate if situation arise. BiPAP pumps air into the small gastric pouch and can lead to complications like breakdown of suture lines, bowel perforation and gastric distension. Though one small study of 27 patients didn't show either any complication or advantage of BiPAP in the first 24 postoperative hours of severely obese patients with comorbid illnesses who have undergone elective gastric bypass 1 but there are case reports in literature showing potential complication and geniune concern for use of of bi-level positive airway pressure after gastric bypass surgery 2.
Reference: click to get abstract/article
1.The effect of bi-level positive airway pressure on postoperative pulmonary function following gastric surgery for obesity - Respiratory Medicine Volume 96, Issue 9, September 2002, Pages 672-676
2. A potential complication of bi-level positive airway pressure after gastric bypass surgery - Obes Surg. 2004 Feb;14(2):282-4.
Tuesday, July 11, 2006
Tuesday July 11, 2006
Paracentesis with seldinger technique / with central venous catheter kit
During paracentesis regular single, double or triple lumen central venous catheter may provide some benefits over angiocath (catheter over needle). Using regular central venous catheter kit's needle, advance till you get ascitic fluid. Now pass J-wire through needle upto appropriate length ------->remove the needle ----> advance your catheter over wire -----> remove the wire ----> if you don't see fluid, slowly pull back the catheter till you get flow. Advantages of this technique:
1) This is relatively safe as paracentesis needle in available kits are usually long and may carry risk of trauma if you keep advancing at non-ascitic area. (In commercial kits, usual length of catheter and needle is about 19 cm/ 7.5 inches).
2) While advancing catheter away from needle, it may get kinked. Catheter getting advanced over wire is unlikely to get kinked.
3) Use catheter from original kit as it may provide advantage of bigger diameter but in large fluid removal you may use tripple lumen catheter and leave it lock like regular central line for 4/5 days to drain required fluid everyday.
4) Multiple ports may allow you to drain in 2/3 bags/bottles simultaneously.
Editors' note: Contributor of this peal is a practicing intensivist but request to hold his and institution's name. We often post bedside tips which are fully anecdotal and individual's idea and may not be evidence based. Use it per your discretion.
Paracentesis with seldinger technique / with central venous catheter kit
During paracentesis regular single, double or triple lumen central venous catheter may provide some benefits over angiocath (catheter over needle). Using regular central venous catheter kit's needle, advance till you get ascitic fluid. Now pass J-wire through needle upto appropriate length ------->remove the needle ----> advance your catheter over wire -----> remove the wire ----> if you don't see fluid, slowly pull back the catheter till you get flow. Advantages of this technique:
1) This is relatively safe as paracentesis needle in available kits are usually long and may carry risk of trauma if you keep advancing at non-ascitic area. (In commercial kits, usual length of catheter and needle is about 19 cm/ 7.5 inches).
2) While advancing catheter away from needle, it may get kinked. Catheter getting advanced over wire is unlikely to get kinked.
3) Use catheter from original kit as it may provide advantage of bigger diameter but in large fluid removal you may use tripple lumen catheter and leave it lock like regular central line for 4/5 days to drain required fluid everyday.
4) Multiple ports may allow you to drain in 2/3 bags/bottles simultaneously.
Editors' note: Contributor of this peal is a practicing intensivist but request to hold his and institution's name. We often post bedside tips which are fully anecdotal and individual's idea and may not be evidence based. Use it per your discretion.
Monday, July 10, 2006
Monday July 10, 2006
Q; How much intavenous albumin should be given to patient while removing ascitic fluid via paracentesis?
A; Per 2004 guidelines published in Hepatology 2004 Mar;39(3):841-56, for management of adult patients with ascites due to cirrhosis by Practice Guidelines Committee, American Association for the Study of Liver Diseases (AASLD),
"Post-paracentesis albumin infusion may not be necessary for a single paracentesis of less than 4 to 5 L. For large-volume paracenteses, an albumin infusion of 8 to 10 g per liter of fluid removed can be considered". (Grade II-2 evidence - Cohort or case-control analytic studies).
Read full guidelines here
Q; How much intavenous albumin should be given to patient while removing ascitic fluid via paracentesis?
A; Per 2004 guidelines published in Hepatology 2004 Mar;39(3):841-56, for management of adult patients with ascites due to cirrhosis by Practice Guidelines Committee, American Association for the Study of Liver Diseases (AASLD),
"Post-paracentesis albumin infusion may not be necessary for a single paracentesis of less than 4 to 5 L. For large-volume paracenteses, an albumin infusion of 8 to 10 g per liter of fluid removed can be considered". (Grade II-2 evidence - Cohort or case-control analytic studies).
Read full guidelines here
Sunday, July 09, 2006
Sunday July 9, 2006
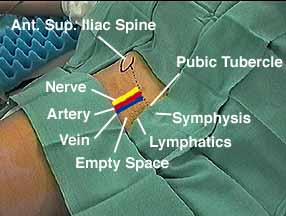
NAVEL
“NAVEL" is a mnemonic for position of the structures at the inguinal ligament, from lateral to medial. It is always helpful to stand beside patient before attempting femoral central line and say NAVEL and try to feel femoral artery and visualize femoral vein before putting needle. Again!, at the inguinal ligament, from lateral to medial
- Femoral Nerve
- Femoral Artery
- Femoral Vein
- Empty space
- Lymphatics
Saturday, July 08, 2006
Saturday July 8, 2006
Q: 21 year old male presented to ER with chest pain. CXR showed small spontaneous pneumothorax with less than 3 cm from apex to cupola. Saturation is 99% on room-air. Management is ?
A) Observation
B) Observation with oxygen
C) Aspiration of the pneumothorax
D) Aspiration of the pneumothorax with application of Heimlich valve or a water seal device
E) Chest tube to suction
Ans. is B (or A)
Clinically stable patient with small primary pneumothorax with less than 3 cm from apex to cupola, should be observed. There is some evidence available that administration of oxygen may speed up resolution of the pneumothorax (exercise caution in patients with COPD).
Read 2 guidelines for management of spontaneous pneumothorax:
1) An American College of Chest Physicians Delphi Consensus Statement Chest. 2001;119:590-602
2) BTS guidelines for the management of spontaneous pneumothorax Thorax 2003;58:ii39
Q: 21 year old male presented to ER with chest pain. CXR showed small spontaneous pneumothorax with less than 3 cm from apex to cupola. Saturation is 99% on room-air. Management is ?
A) Observation
B) Observation with oxygen
C) Aspiration of the pneumothorax
D) Aspiration of the pneumothorax with application of Heimlich valve or a water seal device
E) Chest tube to suction
Ans. is B (or A)
Clinically stable patient with small primary pneumothorax with less than 3 cm from apex to cupola, should be observed. There is some evidence available that administration of oxygen may speed up resolution of the pneumothorax (exercise caution in patients with COPD).
Read 2 guidelines for management of spontaneous pneumothorax:
1) An American College of Chest Physicians Delphi Consensus Statement Chest. 2001;119:590-602
2) BTS guidelines for the management of spontaneous pneumothorax Thorax 2003;58:ii39
Friday, July 07, 2006
Friday July 7, 2006
Q: Which antibiotic interferes with the measurement of serum creatinine and cause "pseudo-acute renal failure" ?
Ans: Cefoxitin: Cefoxitin effects routine measurement of serum creatinine, resulting in falsely elevated levels of renal function. Cefoxitin is a second generation wide spectrum cephalosporin. Other medications which can interfere includes methyldopa and levodopa.
Q: Which antibiotic interferes with the measurement of serum creatinine and cause "pseudo-acute renal failure" ?
Ans: Cefoxitin: Cefoxitin effects routine measurement of serum creatinine, resulting in falsely elevated levels of renal function. Cefoxitin is a second generation wide spectrum cephalosporin. Other medications which can interfere includes methyldopa and levodopa.
Thursday, July 06, 2006
Thursday, July 6, 2006
Case: 54 year old essentially healthy female admitted to floor with abdominal pain, and found to have only constipation as all major workup reported negative. Primary care physician wrote for fleet enemas till constipation get resolved. You have been called as patient was found in bed having "seizure like symptoms"(which you later diagnosed as tetany). On arrival, you found monitor showing arrhythmias and systolic BP in 70s. You asked for STAT labs, started IVF bolus and pressor. Lab shows phophate level of 12 mg/dl (3.87 mmol/L), magnesium of 0.8 meq/L (0.4 mmol/L) and calcium of 4.5 meq/L (2.25 mmol/L)and Cr of 2.4 mg/dl (pt. had normal kidney function on admission). Patient recovered as electrolytes were replaced and kidney function recovered with hemodynamic support.
Ans: Enema induced hyperphosphatemia
The Fleet enema contains 19 g of monobasic sodium phosphate and 7 g of dibasic sodium phosphate per 118 mL of fluid. If series of enemas given, inorganic phosphate salts can readily get absorbed from the gastrointestinal tract and can cause hyperphosphatemia even in patients with normal kidneys. Severe hyperphosphatemia results in acute hypocalcemia and hypomagnesemia. Tetany, seizures, bradycardia prolonged QT interval, dysrhythmias, coma, and cardiac arrest are the possible consequences. Treatment is supportive and replacement of electrolytes. Dialysis may be needed if other measures fail.
Case: 54 year old essentially healthy female admitted to floor with abdominal pain, and found to have only constipation as all major workup reported negative. Primary care physician wrote for fleet enemas till constipation get resolved. You have been called as patient was found in bed having "seizure like symptoms"(which you later diagnosed as tetany). On arrival, you found monitor showing arrhythmias and systolic BP in 70s. You asked for STAT labs, started IVF bolus and pressor. Lab shows phophate level of 12 mg/dl (3.87 mmol/L), magnesium of 0.8 meq/L (0.4 mmol/L) and calcium of 4.5 meq/L (2.25 mmol/L)and Cr of 2.4 mg/dl (pt. had normal kidney function on admission). Patient recovered as electrolytes were replaced and kidney function recovered with hemodynamic support.
Ans: Enema induced hyperphosphatemia
The Fleet enema contains 19 g of monobasic sodium phosphate and 7 g of dibasic sodium phosphate per 118 mL of fluid. If series of enemas given, inorganic phosphate salts can readily get absorbed from the gastrointestinal tract and can cause hyperphosphatemia even in patients with normal kidneys. Severe hyperphosphatemia results in acute hypocalcemia and hypomagnesemia. Tetany, seizures, bradycardia prolonged QT interval, dysrhythmias, coma, and cardiac arrest are the possible consequences. Treatment is supportive and replacement of electrolytes. Dialysis may be needed if other measures fail.
Wednesday, July 05, 2006
Wednesday, July 5, 2006
SPECT as a 'gold standard' to determine Brain Death ?
Angiography has been considered the gold standard for diagnosis of Brain Death for decades. With arrival of new technologies, we try to move more and more towards non-invasive procedures.
Dr. Munari from Italy looked into 20 clinically brain dead patients. ( 99mTc-HMPAO) SPECT and four-vessel angiography were performed in the same session, with no time delay in between. Then, the results of SPECT and angiography were interpreted separately by a specialist in nuclear medicine and a neuroradiologist, respectively; both of them were blind to the results of the other investigation. Both angiography and SPECT confirmed BD in 19 of 20 patients: angiography showed the absence of filling of intracranial arteries, while SPECT showed a picture of empty skull. For one patient, angiography showed slight and late filling of vessels while SPECT showed faint traces of uptake.For this patient, the tests were repeated 48 hrs later, and both showed the arrest of intracranial circulation, thus confirming brain death.
SPECT = Single Photon Emission Computed Tomography
It was concluded by the authors that: SPECT is a good candidate for the gold standard of diagnosis as:
Brain death determination (Source MGH stroke service)
Pre-Apnea test checklist (sample from virginia.edu)
Post-Apnea test checklist (sample from virginia.edu)
References: click to get abstract/article
1. Confirmatory tests in the diagnosis of brain death: Comparison between SPECT and contrast angiography - Critical Care Medicine. 33(9):2068-2073, September 2005
SPECT as a 'gold standard' to determine Brain Death ?
Angiography has been considered the gold standard for diagnosis of Brain Death for decades. With arrival of new technologies, we try to move more and more towards non-invasive procedures.
Dr. Munari from Italy looked into 20 clinically brain dead patients. ( 99mTc-HMPAO) SPECT and four-vessel angiography were performed in the same session, with no time delay in between. Then, the results of SPECT and angiography were interpreted separately by a specialist in nuclear medicine and a neuroradiologist, respectively; both of them were blind to the results of the other investigation. Both angiography and SPECT confirmed BD in 19 of 20 patients: angiography showed the absence of filling of intracranial arteries, while SPECT showed a picture of empty skull. For one patient, angiography showed slight and late filling of vessels while SPECT showed faint traces of uptake.For this patient, the tests were repeated 48 hrs later, and both showed the arrest of intracranial circulation, thus confirming brain death.
SPECT = Single Photon Emission Computed Tomography
It was concluded by the authors that: SPECT is a good candidate for the gold standard of diagnosis as:
- It is noninvasive and, therefore, free from complications and can be repeated for patients who are not brain dead with no harm;
- It shows a clear-cut picture of empty skull, an image that can be easily understood by physicians and even by patient's relatives;
- It fully fits the definition of whole Brain death, showing the absence of whole brain perfusion, down to the foramen magnum.
See interesting Power point presentation on
Brain Death: The Neurologist's Perspective from Stephen T. Mernoff, MD, Clinical Assistant Professor of Neurology, Brown Medical School. Also see our neurology section for various related topics asBrain death determination (Source MGH stroke service)
Pre-Apnea test checklist (sample from virginia.edu)
Post-Apnea test checklist (sample from virginia.edu)
References: click to get abstract/article
1. Confirmatory tests in the diagnosis of brain death: Comparison between SPECT and contrast angiography - Critical Care Medicine. 33(9):2068-2073, September 2005
Tuesday, July 04, 2006
Happy Birthday America
How many attempts to intubate?
Its hard to give up procedure if you are failing it !!. For intubation, ASA (American Society of Anesthesiologists) recommends to limit laryngoscopic attempts to three. Dr. Thomas C. Mort from Hartford Hospital, CT entered 2833 Critically-ill patients, suffering from cardiovascular, pulmonary, metabolic, neurologic, or trauma-related deterioration into an emergency intubation quality improvement database. Data confirmed that the number of laryngoscopic attempts were directly proportional with the incidence of airway and hemodynamic adverse events (more than 2 attempts).
References: click to get abstract/article
1. Emergency tracheal intubation: complications associated with repeated laryngoscopic attempts - Anesth Analg 2004;99:607-613
How many attempts to intubate?
Its hard to give up procedure if you are failing it !!. For intubation, ASA (American Society of Anesthesiologists) recommends to limit laryngoscopic attempts to three. Dr. Thomas C. Mort from Hartford Hospital, CT entered 2833 Critically-ill patients, suffering from cardiovascular, pulmonary, metabolic, neurologic, or trauma-related deterioration into an emergency intubation quality improvement database. Data confirmed that the number of laryngoscopic attempts were directly proportional with the incidence of airway and hemodynamic adverse events (more than 2 attempts).
- incidence of hypoxemia went from 11.8% to 70%,
- incidence of regurgitation of gastric contents went from 1.9% to 22%,
- incidence of aspiration of gastric contents went from 0.8% to 13%,
- incidence of bradycardia went from 1.6% to 21%, and
- incidence of cardiac arrest went from 0.7% to 11%
Call for help !! and remember, to limit intubation attempts to 3, unless untill you are trained to deal with 'difficult intubations'.
References: click to get abstract/article
1. Emergency tracheal intubation: complications associated with repeated laryngoscopic attempts - Anesth Analg 2004;99:607-613
Monday, July 03, 2006
 Monday July 3, 2006
Monday July 3, 2006Simplify D-dimer
D-dimer has great negative predictive value in excluding pulmonary embolism (PE) or deep vein thrombosis (DVT). So far we had to send blood for laboratory-based quantitative D-dimer.
Simplify D-dimer is a new version of test which can be performed at bedside quickly and can provide instant clue 1. Check here to see details on test, that can be performed with a drop of blood at bedside.
Recently in chest, Dr. Kline and coll. from Department of Emergency Medicine, Carolinas Medical Center, Charlotte, NC reported that the posttest prevalence of PE among low-risk patients with negative d-dimer results by simplify D-dimer Assay was only 0.7% 2, supplementing the previous famous study on d-dimer by Dr. Wells 3.
Related previous pearls:
Wells Score of DVT ,
What if even thrombolysis fails in massive PE ?
References: click to get abstract/article
1. A new rapid bedside assay for D-dimer measurement (Simplify D-dimer) in the diagnostic work-up for deep vein thrombosis - J Thromb Haemost. 2003 Dec;1(12):2681-3.
2. Prospective Study of the Diagnostic Accuracy of the Simplify D-dimer Assay for Pulmonary Embolism in Emergency Department Patients Chest. 2006;129:1417-1423.)
3. Excluding Pulmonary Embolism at the Bedside without Diagnostic Imaging: Management of Patients with Suspected Pulmonary Embolism Presenting to the Emergency Department by Using a Simple Clinical Model and D-dimer - 17 July 2001 Volume 135 Issue 2 Pages 98-107, Annals
Sunday, July 02, 2006
BNP
Sunday July 2, 2006
So what is the cut off of BNP ?
When the landmark article on BNP published in The New England Journal of Medicine in July 2002 1, the cutoff point in establishing or excluding the diagnosis of congestive heart failure in patients with acute dyspnea was given at 100 pg per milliliter. But over time we learned that this level probably carries more negative predictive value and there may be a huge gray zone before a definite high BNP value, atleast in critical care setting. This month in Critical Care Medicine 2, Dr. Rana and coll. from Mayo Clinic College of Medicine, Rochester, MN looked into this gray zone. Their conclusion:
"When measured early after the onset of acute pulmonary edema, a BNP level of less than 250 pg/mL supports the diagnosis of acute lung injury. The high rate of cardiac and renal dysfunction in critically ill patients limits the discriminative role of BNP. No level of BNP could completely exclude cardiac dysfunction".
The median time from the onset of pulmonary edema to BNP testing was 3 hrs.
Other interesting findings in the study:
* The predictive value of BNP in the differentiation between ALI and cardiogenic pulmonary edema was comparable with PAOP (when measured) and superior to troponin and echocardiographic determination of ejection fraction. (Not supported by other studies - see related peal below).
*The accuracy of BNP improved if pts with renal failure were excluded.
* BNP levels of more than 950 pg/dL suggest congestive heart failure and BNP levels of less than 250 suggest ALI, the values in between have no diagnostic value.
Related previous pearls:
BNP or Pro-BNP ? Re. Nesiritide (Netrecor)
So what is the cut off of BNP ?
When the landmark article on BNP published in The New England Journal of Medicine in July 2002 1, the cutoff point in establishing or excluding the diagnosis of congestive heart failure in patients with acute dyspnea was given at 100 pg per milliliter. But over time we learned that this level probably carries more negative predictive value and there may be a huge gray zone before a definite high BNP value, atleast in critical care setting. This month in Critical Care Medicine 2, Dr. Rana and coll. from Mayo Clinic College of Medicine, Rochester, MN looked into this gray zone. Their conclusion:
"When measured early after the onset of acute pulmonary edema, a BNP level of less than 250 pg/mL supports the diagnosis of acute lung injury. The high rate of cardiac and renal dysfunction in critically ill patients limits the discriminative role of BNP. No level of BNP could completely exclude cardiac dysfunction".
The median time from the onset of pulmonary edema to BNP testing was 3 hrs.
Other interesting findings in the study:
* The predictive value of BNP in the differentiation between ALI and cardiogenic pulmonary edema was comparable with PAOP (when measured) and superior to troponin and echocardiographic determination of ejection fraction. (Not supported by other studies - see related peal below).
*The accuracy of BNP improved if pts with renal failure were excluded.
* BNP levels of more than 950 pg/dL suggest congestive heart failure and BNP levels of less than 250 suggest ALI, the values in between have no diagnostic value.
Related previous pearls:
References: click to get abstract/article
1. Rapid Measurement of B-Type Natriuretic Peptide in the Emergency Diagnosis of Heart Failure - July 18, 2002,N Engl J Med 2002; 347:161-167, Jul 18, 2002
2. B-type natriuretic peptide in the assessment of acute lung injury and cardiogenic pulmonary edema - Critical Care Medicine. 34(7):1941-1946, July 2006.
Saturday, July 01, 2006
Elevation of the head of the bed- 30 or 45 degrees ?
Answer is probably 45 degrees.Elevation of the head of the bed is a must thing in ICU, unless some contra-indication. It is an essential part of VAP (ventilator associated pneumonia) bundle. But there is some debate about the extent of elevation need to be done. Accepted level is atleast 30 degrees but many guidelines wrote for 45 degrees. IHI recommends elevation anywhere from 30 to 45 degrees 3.
Study from The Netherlands 1 compared 109 patients in the supine group to 112 in the semirecumbent group. Target for semirecumbent group was 45 degrees but the targeted backrest elevation of 45° for semirecumbent positioning was not reached, so supine position (10°) was compared with achieved semirecumbent positioning (28°). Elevation of head of bed to 28° did not prevent the development of VAP.
7 years back Drakulovic and coll. published their landmark study in lancet showing 83% decrease of bacteriologically confirmed VAP in a group of patients treated in a semirecumbent position of 45° 2.
So the answer is probably 45 degrees or to be diplomatically right - atleast more than 30 degrees.
But is it easy to do and keep head of bed elevated to 45 degrees in practical world ?. The study group found that despite the presence of dedicated research nurses to control and maintain patient positioning, the semirecumbent treatment position with an aimed backrest elevation of 45° is not feasible for mechanically ventilated patients.
Another interesting question raised in discussion of first study: Is semirecumbent positioning itself a risk for VAP ? !!!, as pooling of colonized oropharyngeal fluids above the inflated cuff of the endotracheal tube is common in mechanically ventilated patients and it is possible that the semirecumbent position (and all movements to keep it) stimulates leakage of oropharyngeal fluid by means of gravity. Whether ETT with continuous aspiration of subglottic secretions (CASS) will be more effective than semirecumbent positioning?
References: Click to get article/abstract
1. Feasibility and effects of the semirecumbent position to prevent ventilator-associated pneumonia: A randomized study - Critical Care Medicine. 34(2):396-402, February 2006.
2. Supine body position as a risk factor for nosocomial pneumonia in mechanically ventilated patients: a randomised trial - Lancet.1999 Nov 27;354(9193):1851-8.
3. Elevation of the Head of the Bed - Institute for Healthcare Improvement
Friday, June 30, 2006
Friday June 30, 2006
Double the dose of mucomyst ?
A noteworthy study came out yesterday in The New England Journal of Medicine1 regarding protective effect of N-Acetylcysteine in Contrast-Induced Nephropathy in primary angioplasty. When the cumulative dose of N-Acetylcysteine was doubled from 3000 mg (a 600mg IV bolus before angioplasty followed by 600 mg orally twice daily for the 48 hours after angioplasty) to 6000 mg (a 1200 mg IV bolus followed by 1200 mg orally twice daily for the 48 hours after intervention), it showed
Double the dose of mucomyst ?
A noteworthy study came out yesterday in The New England Journal of Medicine1 regarding protective effect of N-Acetylcysteine in Contrast-Induced Nephropathy in primary angioplasty. When the cumulative dose of N-Acetylcysteine was doubled from 3000 mg (a 600mg IV bolus before angioplasty followed by 600 mg orally twice daily for the 48 hours after angioplasty) to 6000 mg (a 1200 mg IV bolus followed by 1200 mg orally twice daily for the 48 hours after intervention), it showed
- significant decrease in increase of serum creatinine concentration (15 percent vs 8 percent)
- overall decrease in in-hospital mortality in patients with contrast induced nephropathy (4 percent vs 3 percent).
- When the combined end point of death, acute renal failure requiring temporary renal replacement therapy, or the need for ventilator during the acute phase of myocardial infarction was considered, the rate was 7% in the standard dose group, and 5% in the high dose group.
In study there were 3 groups - placebo, standard dose and double dose.
It appears that, the benefit of high-dose N-acetylcysteine is greater in patients receiving a larger or more than regular volume of contrast.
Conclusion: N-acetylcysteine reduced the severity of contrast medium induced nephropathy in patients with acute myocardial infarction treated with primary angioplasty. The effect appears to be dose dependent and is accompanied by a significantly improved in-hospital outcome.
Related previous pearls:
Contrast induced Nephropathy and
Preventing contrast-Induced Nephropathy
Reference: Click to get article/abstract
1. N-Acetylcysteine and Contrast-Induced Nephropathy in Primary Angioplasty - Volume 354:2773-2782, Number 26, June 29 2006
2. Contrast Nephropathy Prevention With N-Acetylcysteine in Acute Myocardial Infarction - clinicaltrials.gov
Thursday, June 29, 2006

Thursday June 29, 2006
ICU Index Spider Diagram
The Society of Critical Care Medicine’s (SCCM) Coalition for Critical Care Excellence (CCCE) has developed The ICU Index™ (click to get more details) as a measurement tool that can be used at the individual ICU level to baseline a series of performance variables and then track progress. It look into 16 important measures and can either be approached in a regular bar chart form or as a spider diagram.
Goal is to move the said measure as much as possible inside the spider to central target. Comparing spider diagrams every few months can tell improvements in ICU in just one glance. See the diagram above. You may wish to change, add, substract measures like you can track VAP rate, LOS etc as per your local ICU need.
If you would like more information, or would like to participate in the pilot project, please email ICUIndex@sccm.org.
Wednesday, June 28, 2006
Diagnostic criteria of Delirium
Wednesday June 28, 2006
Diagnostic criteria of Delirium
Q: What are 4 basic criteria to label patient as having Delirium?
Related previous pearls:
Zolpidem-Induced Delirium ,
SEROTONIN SYNDROME ,
Amiodarone Neurotoxicity
Diagnostic criteria of Delirium
Q: What are 4 basic criteria to label patient as having Delirium?
A: Per American Psychiatric Association's Diagnostic and Statistical Manual of Mental Disorders. 4th ed. (DSM-IV), Patient is having delirium if
1. Disturbance of consciousness (eg, reduced clarity of awareness of the environment) with reduced ability to focus, sustain, or shift attention.
2. A change in cognition such as memory deficit, disorientation, language disturbance (or the development of a perceptual disturbance that is not better accounted for by a preexisting, established, or evolving dementia).
3. The disturbance develops over a short period of time (usually hours) and tends to fluctuate during the course of the day.
4. Disturbance caused by a general medical condition or substance intoxication or medication use.
Related website:
Related previous pearls:
Zolpidem-Induced Delirium ,
SEROTONIN SYNDROME ,
Amiodarone Neurotoxicity
References: click to get abstract/article
1. An Empirical Study of Different Diagnostic Criteria for Delirium Among Elderly Medical Inpatients - J Neuropsychiatry Clin Neurosci 15:200-207, May 2003
2. Delirium in Elderly Patients - Focus 3:320-332 (2005)
3. Delirium in Older Persons - N. Engl. J. Med., March 16, 2006; 354(11): 1157 - 1165
4. Delirium - emedicine.com
5. Delirium - American Family Physician® Vol. 67/No. 5 (March 1, 2003)
Tuesday, June 27, 2006
Tuesday June 27, 2006
We will need more intensivists !!
Currently in USA, only 37% of critically ill patients are cared for by intensivists and an estimated 360,000 deaths occur each year in ICUs not managed by intensivists. In 2003, the US Senate asked Health Resources and Services Administration (HRSA) to work with the American College of Chest Physicians (ACCP) to update critical care workforce models in order to more accurately assess the adequacy of supply for critical care physicians. In the newly released US Department of Health and Human Services Report to Congress: The Critical Care Workforce: A Study of the Supply and Demand for Critical Care Physicians, it has been predicted that the demand for critical care services will increase rapidly, while the intensivist supply would not be able to care for a greater proportion of critically ill patients. The shortage is will be exacerbated by the year 2020 due to the aging population and the increased utilization of intensivists.
By 2020, the demand for intensivists would likely increase by 129 percent above the current supply.
Some Suggestions include:
We will need more intensivists !!
Currently in USA, only 37% of critically ill patients are cared for by intensivists and an estimated 360,000 deaths occur each year in ICUs not managed by intensivists. In 2003, the US Senate asked Health Resources and Services Administration (HRSA) to work with the American College of Chest Physicians (ACCP) to update critical care workforce models in order to more accurately assess the adequacy of supply for critical care physicians. In the newly released US Department of Health and Human Services Report to Congress: The Critical Care Workforce: A Study of the Supply and Demand for Critical Care Physicians, it has been predicted that the demand for critical care services will increase rapidly, while the intensivist supply would not be able to care for a greater proportion of critically ill patients. The shortage is will be exacerbated by the year 2020 due to the aging population and the increased utilization of intensivists.
By 2020, the demand for intensivists would likely increase by 129 percent above the current supply.
Some Suggestions include:
- Increase role of eICU
- Possible rationing of critical care services or regionalization of ICU services like trauma system
- Restructuring current Medicare reimbursement system
- Expanding National Health Services Corps and J-1 waiver program
- Only deserving patients getting admission to ICU
- Decreasing care for know futile outcomes by more public/physician education
Read full report:
HRSA Report to Congress. The Critical Care Workforce: A Study of the Supply and Demand for Critical Care PhysiciansMonday, June 26, 2006
Monday June 26, 2006
Thrombelastography - TEG
TEG was first introduced about 60 years ago by Hartert . TEG monitors hemostasis as a whole dynamic process and measures the viscoelastic properties of blood. The strength of a clot is graphically represented over time in a cigar shape figure. With little practice, just a glance at shape and size of cigar, it provides clue to underlying disease process. It is an underutilized tool in ICU. See picture for self explanation:
Read review on Thromboelastography/thromboelastometry here (pdf file) (ref: Clin. Lab. Haem. 2005, 27, 81–90)
Sunday, June 25, 2006
Sunday June 25, 2006
Introducing iCritical Care Podcasts
www.sccm.org/podcast
iCritical Care Podcasts from Society of Critical Care Medicine is a kind of radio which you can listen on your home computer, or your portable media player (iPod and others). The iCritical Care Podcast is a novel way for you to keep up-to-date with the latest in Critical Care. Site get frequently updated with talks on recent breakthrough articles carrying interviews with authors of these articles as well as talks on non-academic but critical care related issues. So far upto 34 talks have been added including but not limited to:
Introducing iCritical Care Podcasts
www.sccm.org/podcast
iCritical Care Podcasts from Society of Critical Care Medicine is a kind of radio which you can listen on your home computer, or your portable media player (iPod and others). The iCritical Care Podcast is a novel way for you to keep up-to-date with the latest in Critical Care. Site get frequently updated with talks on recent breakthrough articles carrying interviews with authors of these articles as well as talks on non-academic but critical care related issues. So far upto 34 talks have been added including but not limited to:
- Lorazepam vs. Propofol
- Catheter-Related Bloodstream Infections
- Prophylactic Antimicrobial Use in the ICU
- Hospital Mortality Assessment
- Rationing in the ICU
- Morbid Obesity and the Surgical Critical Patient
- Dopamine's Influence on the Outcome of Shock
- Defining and Treating Abdominal Compartment Syndrome
- Early Indicators of Sepsis Survival
- Getting Our ICU Language Straight
- Critical Care Pharmacists
- Implementing the Surviving Sepsis Campaign
Host is
Richard H. Savel, MD, Associate Director, Surgical Intensive Care Unit at Maimonides Medical Center, Brooklyn, NY, and Assistant Professor of Medicine at Mt. Sinai School of Medicine, NY.Again site is www.sccm.org/podcast
Related previous themes:
Introducing Resident ICU Course and
PACT - Critical Care distant learning course
Saturday, June 24, 2006
fenoldopam
Saturday June 24, 2006
Case: 39 year old male admitted with hypertensive emergency after he ran out of his prescriptions. "ED Doc" started patient on IV cardene (nicardipine) drip and resumed patient's home med for BP which consist of Toprol (metoprolol) XL - first dose given in ER. On review of CXR you noticed some pulmonary edema and decide to switch to Fenoldopam to get dual effect of lowering BP as well as dopaminergic effect to resolve pulmonary edema. Patient dropped his BP precipitously and coded.
Probable cause: It is not advisable to start fenoldopam on patients with B-blocker or atleast close caution should be maintained. Concomitant use of beta-blockers in conjunction with fenoldopam may cause life threatening hypotension from beta-blocker's inhibition of the sympathetic reflex response to fenoldopam 1.
Related previous pearl: Renal dose Fenoldopam ?
References: click to get abstract/article1. Corlopam - fda.gov
2. Fenoldopam — A Selective Peripheral Dopamine-Receptor Agonist for the Treatment of Severe Hypertension - Volume 345:1548-1557, Number 21, Nov. 22,2001
Case: 39 year old male admitted with hypertensive emergency after he ran out of his prescriptions. "ED Doc" started patient on IV cardene (nicardipine) drip and resumed patient's home med for BP which consist of Toprol (metoprolol) XL - first dose given in ER. On review of CXR you noticed some pulmonary edema and decide to switch to Fenoldopam to get dual effect of lowering BP as well as dopaminergic effect to resolve pulmonary edema. Patient dropped his BP precipitously and coded.
Probable cause: It is not advisable to start fenoldopam on patients with B-blocker or atleast close caution should be maintained. Concomitant use of beta-blockers in conjunction with fenoldopam may cause life threatening hypotension from beta-blocker's inhibition of the sympathetic reflex response to fenoldopam 1.
Related previous pearl: Renal dose Fenoldopam ?
References: click to get abstract/article1. Corlopam - fda.gov
2. Fenoldopam — A Selective Peripheral Dopamine-Receptor Agonist for the Treatment of Severe Hypertension - Volume 345:1548-1557, Number 21, Nov. 22,2001
Friday, June 23, 2006
Friday June 23, 2006
Case: 24 year old male admitted with left thigh cellulitis and abcess. I and D was performed and cefazolin (ancef) was initiated. Patient did not respond to cefazolin and antibiotic was changed to vancomycin after availability of sensitivity from micro lab. Patient showed marked improvement over next 3 days except patient complaint of new rash on his body which you attributed to "Red man syndrome" and wrote an order to infuse vancomycin slowly and with increase dilution. Next day, as you reached hospital, you were informed by outgoing intensivist that patient deteriorated overnight and required intubation. You were baffled and as you examine the patient, you find extensive dermal exfoliation along with axillary and inguinal lymphadenopathy. On lab, LDH and liver enzymes were markedly elevated and kidney funtion deteriorated from normal to anuria. CBC showed eosinophilia.
Vancomycin-induced Stevens-Johnson syndrome
Stevens-Johnson syndrome is an acute mucocutaneous process characterized by severe exfoliative dermatitis and mucosal involvement of the gastrointestinal tract and conjunctiva. Pathogenesis is unclear, but an immunological mechanism, probably cell-mediated, has been suggested. Clinical diagnosis of Stevens-Johnson syndrome is based on the presence of "target" or "iris" lesions involving the skin and erosive lesions of two or more mucosal surfaces. Associated findings include extensive dermal exfoliation, nephritis, lymphadenopathy, hepatitis, and multiple serologic abnormalities. Vancomycin, a glycopeptide antibiotic, has case reports in literature produceing immunologically mediated adverse reactions such as interstitial nephritis, linear IgA bullous dermatosis, exfoliative erythroderma, necrotizing cutaneous vasculitis and toxic epidermal necrolysis. The treatment consists of cessation of vancomycin and administration of antihistamine and/or steroid.
See pic here
References: click to get abstract/article
1.Vancomycin-induced Stevens-Johnson syndrome Allergy Asthma Proc. 1996 Mar-Apr;17(2):75-8.
2.Stevens-Johnson-type reaction with vancomycin treatment. - Ann Pharmacother. 1992 Dec;26(12):1520-1
3 Uncommon Vancomycin-Induced Side Effects - Brazilian Journal of Infectious Diseases - 2002;6(4):196-200
Case: 24 year old male admitted with left thigh cellulitis and abcess. I and D was performed and cefazolin (ancef) was initiated. Patient did not respond to cefazolin and antibiotic was changed to vancomycin after availability of sensitivity from micro lab. Patient showed marked improvement over next 3 days except patient complaint of new rash on his body which you attributed to "Red man syndrome" and wrote an order to infuse vancomycin slowly and with increase dilution. Next day, as you reached hospital, you were informed by outgoing intensivist that patient deteriorated overnight and required intubation. You were baffled and as you examine the patient, you find extensive dermal exfoliation along with axillary and inguinal lymphadenopathy. On lab, LDH and liver enzymes were markedly elevated and kidney funtion deteriorated from normal to anuria. CBC showed eosinophilia.
Vancomycin-induced Stevens-Johnson syndrome
Stevens-Johnson syndrome is an acute mucocutaneous process characterized by severe exfoliative dermatitis and mucosal involvement of the gastrointestinal tract and conjunctiva. Pathogenesis is unclear, but an immunological mechanism, probably cell-mediated, has been suggested. Clinical diagnosis of Stevens-Johnson syndrome is based on the presence of "target" or "iris" lesions involving the skin and erosive lesions of two or more mucosal surfaces. Associated findings include extensive dermal exfoliation, nephritis, lymphadenopathy, hepatitis, and multiple serologic abnormalities. Vancomycin, a glycopeptide antibiotic, has case reports in literature produceing immunologically mediated adverse reactions such as interstitial nephritis, linear IgA bullous dermatosis, exfoliative erythroderma, necrotizing cutaneous vasculitis and toxic epidermal necrolysis. The treatment consists of cessation of vancomycin and administration of antihistamine and/or steroid.
See pic here
References: click to get abstract/article
1.Vancomycin-induced Stevens-Johnson syndrome Allergy Asthma Proc. 1996 Mar-Apr;17(2):75-8.
2.Stevens-Johnson-type reaction with vancomycin treatment. - Ann Pharmacother. 1992 Dec;26(12):1520-1
3 Uncommon Vancomycin-Induced Side Effects - Brazilian Journal of Infectious Diseases - 2002;6(4):196-200
Thursday, June 22, 2006
Thursday June 22, 2006
Imipenem and Primaxin
Q: What advantage we have when we add cilastatin with Impenem ?
OR in other words, What is the difference between Imipenem and Primaxin (Imipenem plus Cilastatin) ?
A: Imipenem get metabolized in the kidneys by enzyme called dehydropeptidase I and cannot achive therapeutic level in urine. Addition of Cilastatin inhibit the enzyme in kidney's renal tubules so that when imipenem and cilastatin are given concomitantly, increased imipenem levels are achieved in the urine.
Bonus Pearl: Primaxin is hemodialyzable so dose may be unreliable in such patients or preferably should be given after hemodialysis session. Dose in dialysis dependent patient is either 250 mg q 12 hrs or 500 mg after each dialysis.
When Imipenem was introduced, it get reputed with nick name of "Jesus water" due to its broad coverage and to kill most bugs.
Imipenem and Primaxin
Q: What advantage we have when we add cilastatin with Impenem ?
OR in other words, What is the difference between Imipenem and Primaxin (Imipenem plus Cilastatin) ?
A: Imipenem get metabolized in the kidneys by enzyme called dehydropeptidase I and cannot achive therapeutic level in urine. Addition of Cilastatin inhibit the enzyme in kidney's renal tubules so that when imipenem and cilastatin are given concomitantly, increased imipenem levels are achieved in the urine.
Bonus Pearl: Primaxin is hemodialyzable so dose may be unreliable in such patients or preferably should be given after hemodialysis session. Dose in dialysis dependent patient is either 250 mg q 12 hrs or 500 mg after each dialysis.
When Imipenem was introduced, it get reputed with nick name of "Jesus water" due to its broad coverage and to kill most bugs.
Tuesday, June 20, 2006
Wednesday June 21, 2006
Normosol is NOT just Normal Saline
Being an intensivist, the most important thing to know - what is infusing in patient. There is some misconception that Normosol is just another name of Normal Saline, which is not true.
Contents of Normal Saline:
Na = 154 mEq/L
Cl = 154 mEq/L
PH = 5.4
Contents of Normosol:
Na = 140 mEq/L
Cl = 98 mEq/L
K = 4 mEq/L
Mg = 3 mEq/L
Acetate = 27 mEq/LGluconate = 23 mEq/L
PH =6.6
Normosol contains added K and Mg which may be unsuitable for some patients like patients with renal failure.
Bonus Pearl: If it says R on IVF bag, it means manufacturer recommends bag for replacement therapy and if it says M on IVF bag , it is meant for maintenance IV. Contents may be little different. Most "M" bags contain extra dextrose.
Related Previous Pearl: Difference between LR and Normal Saline
Normosol is NOT just Normal Saline
Being an intensivist, the most important thing to know - what is infusing in patient. There is some misconception that Normosol is just another name of Normal Saline, which is not true.
Contents of Normal Saline:
Na = 154 mEq/L
Cl = 154 mEq/L
PH = 5.4
Contents of Normosol:
Na = 140 mEq/L
Cl = 98 mEq/L
K = 4 mEq/L
Mg = 3 mEq/L
Acetate = 27 mEq/LGluconate = 23 mEq/L
PH =6.6
Normosol contains added K and Mg which may be unsuitable for some patients like patients with renal failure.
Bonus Pearl: If it says R on IVF bag, it means manufacturer recommends bag for replacement therapy and if it says M on IVF bag , it is meant for maintenance IV. Contents may be little different. Most "M" bags contain extra dextrose.
Related Previous Pearl: Difference between LR and Normal Saline
Labetolol dose
Tuesday June 20, 2006
Labetolol dose
Q: What is the usual guided dose of labetalol in hypertensive emergency ?
A; Loading dose of 0.25 mg/kg followed by 0.5 mg/kg every 15 minutes but total dose should remain less than 3.25 mg/kg.
Advantage of Labetalol:
- Action within 5 minutes and
- combined alpha and beta blocker effect
Disadvantage of Labetalol:
- It decreases both SVR (Systemic Vascular Resistance) and CO (Cardiac Output).
(From Dr. Joseph Varon's lecture "Hypertensive Emergencies in the Perioperative Cardiovascular Setting" at Hypertensive Crisis: Strategies To minimize End-Organ Damage With Focus On The Heart and Brain - symposium during Chest 2005)
Monday, June 19, 2006
Anemia in ICU
Monday June 19, 2006
Anemia in ICU
Q: If you admit a patient with Hb of 10 g/dL and draw 100 ml of blood for various lab works. How much will be the drop in Hb ?
A; Hb will drop from 10 to 9.3 g/dL. With each 100 ml of blood draws, Hb drop by 0.7 g/dL 1. Remember ! phlebotomy (blood draws) is the major of cause anemia in ICUs.
Bonus pearl: In anemic patients, if blood workup is necessary, use pediatric tubes.
Related previous pearl: ICU anemia score
Reference: click to get abstract
Blood testing causes anemia - J Gen Intern Med 2005; 20:520–524
Anemia in ICU
Q: If you admit a patient with Hb of 10 g/dL and draw 100 ml of blood for various lab works. How much will be the drop in Hb ?
A; Hb will drop from 10 to 9.3 g/dL. With each 100 ml of blood draws, Hb drop by 0.7 g/dL 1. Remember ! phlebotomy (blood draws) is the major of cause anemia in ICUs.
Bonus pearl: In anemic patients, if blood workup is necessary, use pediatric tubes.
Related previous pearl: ICU anemia score
Reference: click to get abstract
Blood testing causes anemia - J Gen Intern Med 2005; 20:520–524
pre-ICU care
Sunday June 18, 2006
To decrease ICU mortality - fix pre-ICU care !!
Team from Cooper University Hospital, Camden, NJ (Raquel Nahra, MD, Christa Schorr, RN and David R. Gerber, DO) - addressed a very important and often ignored issue at ACCP meeting of november 2005 : PRE–INTENSIVE CARE UNIT LENGTH OF STAY AND OUTCOME IN CRITICALLY ILL PATIENTS 1.
Patients were divided into 4 groups:
*HLOS = hospital length of stay and data was obtained from the Project Impact database.
Study found that: ICU admission from a general care floor after more than / = 6 days is associated with poor outcome(Group M2). Suboptimal care prior to ICU admission is the reason for poorer outcomes. Probable reasons:
Editors note: Lessons to be learned include intensivists' early involvement in care outside ICU, formation of rapid response team, close working of floor team (hospitalist) and intensivist and more inservices/training for floor staff.
Related previous pearl: Rapid Response Team
Related Sites: IHI's RRT - getting started kit and SCCM's RRT/ MET forum
Reference: click to get abstract
PRE–INTENSIVE CARE UNIT LENGTH OF STAY AND OUTCOME IN CRITICALLY ILL PATIENTS - Critical Care Outcomes, ACCP meeting November 2, 2005
To decrease ICU mortality - fix pre-ICU care !!
Team from Cooper University Hospital, Camden, NJ (Raquel Nahra, MD, Christa Schorr, RN and David R. Gerber, DO) - addressed a very important and often ignored issue at ACCP meeting of november 2005 : PRE–INTENSIVE CARE UNIT LENGTH OF STAY AND OUTCOME IN CRITICALLY ILL PATIENTS 1.
Patients were divided into 4 groups:
- Group M1 - medical patients HLOS less than / = 5 days
- Group M2 - medical patients HLOS more than / = 6 days
- Group S1 - surgical patients HLOS less than / =5 but more than 1 day
- Group S2 - surgical patients HLOS more than / = 6 days
*HLOS = hospital length of stay and data was obtained from the Project Impact database.
Study found that: ICU admission from a general care floor after more than / = 6 days is associated with poor outcome(Group M2). Suboptimal care prior to ICU admission is the reason for poorer outcomes. Probable reasons:
- Poor organization,
- Insufficient knowledge,
- Failure to appreciate clinical urgency,
- Inadequate supervision and
- Failure to seek advice
Editors note: Lessons to be learned include intensivists' early involvement in care outside ICU, formation of rapid response team, close working of floor team (hospitalist) and intensivist and more inservices/training for floor staff.
Related previous pearl: Rapid Response Team
Related Sites: IHI's RRT - getting started kit and SCCM's RRT/ MET forum
Reference: click to get abstract
PRE–INTENSIVE CARE UNIT LENGTH OF STAY AND OUTCOME IN CRITICALLY ILL PATIENTS - Critical Care Outcomes, ACCP meeting November 2, 2005
Saturday, June 17, 2006
EKG changes in Hyperkalemia
Saturday June 17, 2006
4 EKG changes in Hyperkalemia
The first EKG sign of hyperkalemia is peaked T waves and usually appears once K level go around 6 meq/L.
Second sign is prolongation of PR interval which can be seen with K level going around or above 7 meq/L.
Absent P wave with widen QRS complex is the third manifestation and is a very dangerous sign. It means that atrial activity is lost and stage is set for ventricular tachycardia/fibrillation. It is usually seen at level around 8-9 meq/L.
Ventricular tachycardia/fibrillation is the price you pay of ignoring above changes on monitor.
Above are just rough rules of thumb. Read a good review
Recognising signs of danger: ECG changes resulting from an abnormal serum potassium concentration (source: Emerg Med J 2002; 19:74-77)
4 EKG changes in Hyperkalemia
The first EKG sign of hyperkalemia is peaked T waves and usually appears once K level go around 6 meq/L.
Second sign is prolongation of PR interval which can be seen with K level going around or above 7 meq/L.
Absent P wave with widen QRS complex is the third manifestation and is a very dangerous sign. It means that atrial activity is lost and stage is set for ventricular tachycardia/fibrillation. It is usually seen at level around 8-9 meq/L.
Ventricular tachycardia/fibrillation is the price you pay of ignoring above changes on monitor.
Above are just rough rules of thumb. Read a good review
Recognising signs of danger: ECG changes resulting from an abnormal serum potassium concentration (source: Emerg Med J 2002; 19:74-77)
Friday, June 16, 2006
Friday June 16, 2006
Carvediol (Coreg)
Q: How Carvediol (Coreg) is different from other B-blockers?
A; Coreg is a triple blocker. It blocks beta-1, beta-2 and alpha-1 receptors. Alpha-1 blockade provides vasodilation and so protection in congestive heart failure (CHF). U.S. Carvedilol Heart Failure Study with 1094 patients showed 65% lower risk of death than placebo patients 1. Dose should be started at 3.125 mg BID and titrated (as tolerated) upto 25 mg BID. Obese patients may require higher dose.
Extended release Metoprolol (Toprol XL) is another B-blocker approved from FDA for use in CHF. MERIT-HF study showed 34% reduction in mortality than placebo in patients taking Toprol XL 2.
FDA approves only Toprol-XL and Coreg for CHF.
References: Click to get article/abstract
1. The Effect of Carvedilol on Morbidity and Mortality in Patients with Chronic Heart Failure - N Engl J Med. 1996;334:1349-1355.
2. MERIT-HF Study Group. Effect of metoprolol CR/XL in chronic heart failure: metoprolol CR/XL randomised intervention trial in congestive heart failure. Lancet. 1999;353:2001-2007
Carvediol (Coreg)
Q: How Carvediol (Coreg) is different from other B-blockers?
A; Coreg is a triple blocker. It blocks beta-1, beta-2 and alpha-1 receptors. Alpha-1 blockade provides vasodilation and so protection in congestive heart failure (CHF). U.S. Carvedilol Heart Failure Study with 1094 patients showed 65% lower risk of death than placebo patients 1. Dose should be started at 3.125 mg BID and titrated (as tolerated) upto 25 mg BID. Obese patients may require higher dose.
Extended release Metoprolol (Toprol XL) is another B-blocker approved from FDA for use in CHF. MERIT-HF study showed 34% reduction in mortality than placebo in patients taking Toprol XL 2.
FDA approves only Toprol-XL and Coreg for CHF.
References: Click to get article/abstract
1. The Effect of Carvedilol on Morbidity and Mortality in Patients with Chronic Heart Failure - N Engl J Med. 1996;334:1349-1355.
2. MERIT-HF Study Group. Effect of metoprolol CR/XL in chronic heart failure: metoprolol CR/XL randomised intervention trial in congestive heart failure. Lancet. 1999;353:2001-2007
Wednesday, June 14, 2006
Wednesday June 14, 2006
Swan is still very in !!
Lately we had some constant negative studies for pulmonary artery catheter like ESCAPE trial, PAC-MAN study and recently published ARDSnet's FACTT trial 2.
This month Critical Care Medicine published retrospective database analysis of 53,312 trauma patients 1. After all adjustments following groups showed benefit:
- Patients aged 61-90 yrs,
- with arrival base deficit worse than -11 and
- Injury Severity Score of 25-75.
It was found that it was associated with a protective effect in patients with severe shock, regardless of age, and in older patients with moderate shock.
Also note negative outcome: Highest risk of death associated with PAC use was in younger patients who arrived at the ED without a significant base deficit. Moreover, no survival benefit was detected with PAC use in patients arriving at the ED without evidence of shock.
Conclusion: PAC insertion is associated with
- improved outcome in critically injured patients with severe shock at admission, regardless of age, and
- in elderly patients with moderate shock.
Related previous pearls: PAC-MAN study ! and ESCAPE Trial
Reference: Click to get article
1. Pulmonary artery catheter use is associated with reduced mortality in severely injured patients: A National Trauma Data Bank analysis of 53,312 patients - Critical Care Medicine. 34(6):1597-1601, June 2006.
2. Pulmonary-Artery versus Central Venous Catheter to Guide Treatment of Acute Lung Injury - Volume 354:2213-2224, NEJM, May 25, 2006
Tuesday, June 13, 2006
CVP via PICC
Tuesday June 13, 2006
Can we measure CVP (central venous pressure) with PICCs (peripherally inserted central catheters) ?
YES: PICC lines can be used to measure CVP, if situation arise. CVP recorded via PICC lines are about 1 mm Hg higher than CVP from centrally inserted venous catheters. PICC lines need to be hooked to continuous infusion with heparinized saline at 3 mL/hr to overcome the resistance of longer length and narrower lumen of PICC line. Trend should be followed for better perception as first PICC measured CVP is reported higher, probably due to microthrombi which get flushed later on.
Dr. Black and coll. from Pennsylvania State University College of Medicine, Hershey, PA studied 77 data pairs from 12 patients with measurements recorded at end-expiration. 19-gauge dual-lumen PICCs were used and were zeroed/levelled at right atrium. To overcome the longer length, narrower lumen an so higher inherent resistance, continuous infusion device is used with heparinized saline at 3 mL/hr (like in arterial lines) 1.
Reference: Click to get article
1. Central venous pressure measurements: Peripherally inserted catheters versus centrally inserted catheters - Critical Care Medicine. 28(12):3833-3836, December 2000.
Can we measure CVP (central venous pressure) with PICCs (peripherally inserted central catheters) ?
YES: PICC lines can be used to measure CVP, if situation arise. CVP recorded via PICC lines are about 1 mm Hg higher than CVP from centrally inserted venous catheters. PICC lines need to be hooked to continuous infusion with heparinized saline at 3 mL/hr to overcome the resistance of longer length and narrower lumen of PICC line. Trend should be followed for better perception as first PICC measured CVP is reported higher, probably due to microthrombi which get flushed later on.
Dr. Black and coll. from Pennsylvania State University College of Medicine, Hershey, PA studied 77 data pairs from 12 patients with measurements recorded at end-expiration. 19-gauge dual-lumen PICCs were used and were zeroed/levelled at right atrium. To overcome the longer length, narrower lumen an so higher inherent resistance, continuous infusion device is used with heparinized saline at 3 mL/hr (like in arterial lines) 1.
Reference: Click to get article
1. Central venous pressure measurements: Peripherally inserted catheters versus centrally inserted catheters - Critical Care Medicine. 28(12):3833-3836, December 2000.
Subscribe to:
Posts (Atom)